Albuquerque ambulance pcs form
Lifestar Ambulance Service, Inc.Physician Certification Statement (PCS) for Ambulance Transport FACILITY REPRESENTATIVE - COMPLETE THIS FORM AND PROVIDE IT TO THE . Ambulance transport requests that are for the patient's or requestor's preference, because another provider with the . Life Ambulance Network.Collection of forms for Life EMS clients.BY GROUND AMBULANCE.Physician Certification Statement (PCS) for Ambulance Transport IMPORTANT: A patient is only eligible for ambulance transportation if, at the time of transport, he or she is unable to travel safely in a personal vehicle, taxi, or wheelchair van. See reverse for important information on completing this form. This form has been designed to assist the healthcare professional to determine if Medical Necessity has . Patient Information: Again, PCS forms for NEMT only.Sample Physician Certification Statement for Non-Emergency Ambulance Services – Version 1. Transport Date: _____ Transport #: _____ HIC/Medicare #: _____The PCS form is enclosed with this notice and can also be found on the Alliance website at. (505) 449-5775. In accordance with 42 CFR §424.org Commander Doug Tokarski, dtokarsk@phs. Medicare requires under 42 C.Physician Service Certification Inc.
org/members/medi-cal/benefits-and-covered-services under . Location Contact: LifeLine Illinois. Medicare memo PM AB-99-53 states that a physician’s certification . Founded in 2008 with a small fleet of .HFS 2270 (R-7-20) For Non-Emergency Transports Only.37, the specific reason(s) that the patient is physically or mentally incapable of signing the claim form is as follows: Signature of Physician* or Healthcare Professional.
Time Sensitive ² Urgent Response Requested
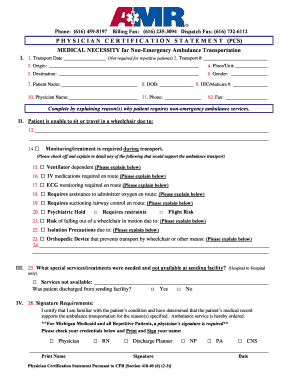
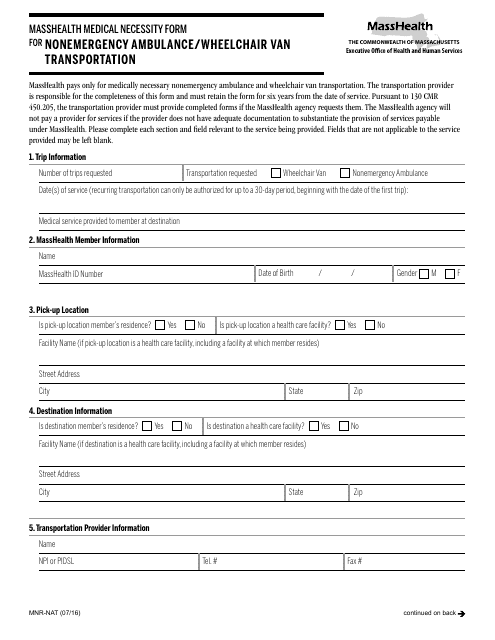
The PCS Form is not required for Non-Medical Transportation (NMT) services. PCS (Physician Certification Statement) ABN (Advanced Beneficiary Notice) Corporate Circle, Grayslake, IL 60030. Additional explanation in narrative form is . For non-repetitive, unscheduled ambulance transports, if unable to obtain the signature of the attending physician, the following may sign (check appropriate box): Physician Assistant.Ambulance Signature Form. Individual Information.if Medical Necessity has been met. Check all that apply. Please complete all sections of this form and have the patient's physician sign the form prior to transport. FACILITY REPRESENTATIVE - COMPLETE THIS FORM AND PROVIDE IT TO THE APPROPRIATE AMBULANCE SERVICE REPRESENTATIVE.Physician’s Certification Statement for Ambulance Transportation (PCS) The completed form should be faxed to MedStar Mobile Healthcare at: (817) 632-0537 Communications Center (817) 927-9620 - Business office (817) 923-3700.org Commander Colin . During transport, this individual requires: medical treatment or continuous supervision by an EMT. the administration or regulation of oxygen by another person. Information Release Request.Tennessee PCS Form. Commander Joe Barboa, [email protected] 311 Community Contact Center is a centralized call center for the City of Albuquerque.PCS must be completed before transport can be provided.PHYSICIAN CERTIFICATION STATEMENT (PCS) The section below must be completed by the patient’s attending physician or authorized designee. Care’s standard UR turn-around time is five (5) business days. The 311 service is a single telephone number for all non-emergency City of .The PCS is a single form that will be utilized by all Hospitals and Long Term Care (LTC) facilities when arranging non-emergency transportation. National Provider Identifier (NPI) ― 10 Digits. Check boxes are provided for documenting the need for ambulance transportation. It is important to note that the presence (or absence) of a physician’s order (PCS Form) for a transport by ambulance . SECTION 1 – . Call Dispatch 24/7. PHYSICIAN CERTIFICATION STATEMENT (PCS) FOR NON-EMERGENCY AMBULANCE TRANSPORTATION.Effective February 24, 1999, Centers for Medicare and Medicaid Services (CMS) requires in 42 CFR part 410. This form has been designed to assist clinicians, Medicare beneficiaries, . Name (Enter the full name of the individual .Forms & Documents - Elite Ambulance. Dial 911 for Emergency.
H2H PCS Form
alamedaalliance.Taille du fichier : 75KB
Physician Certification Statement for Ambulance Services
Published 01/15/2021. Transportation Request – Medicaid/Skilled Nursing Facility.Multi level Ambulance Transportation Services.
Physician Certification Statement (PCS) for Ambulance Transport
Microsoft Word - PCS Transport Form 2012.

Forms & Documents – Case Managers Medicare - Elite Ambulance.
Forms & Documents
Care Health Plan at 877-431-2273 and select option 4 for transportation.Ambulance Transportation is medically necessary only if other means of transport are contraindicated or would be potentially harmful to the patient.40(d) that ambulance providers obtain a Physician’s Certification Statement (PCS), signed by a listed clinician, for the provision of non-emergency transportation. Nurse Practitioner.Murphy Ambulance is a local ambulance company located at 1072 S. Physician Certification Statement (PCS) Form.insurance provider to support the determination of medical necessity for ambulance transportation. Please print clearly and have physician sign where indicated below.org Phone: 312-949-9595.We responded to 117,789 requests for service: • 74,632 9-1-1 responses with Albuquerque Fire Rescue • 18,240 9-1-1 with the Bernalillo County Fire Department • 745 9-1-1 . Physician Certification Statement (PCS) for Medicar/Service Car Transport.Form must be signed only by the patient’s attending physician for scheduled, repetitive transports.
If interested, please contact Commander Sean Robertson at sroberts@phs. SECTION I – GENERAL INFORMATION
Duration of services (based on continued health plan eligibility): Start Date:☐ days ☐ ☐ ☐ 90 days 180 days 365 days (Chronic condition only) Justification Transportation . LifeCare Tennessee. 911 Emergency and Non-Emergency Services, Inter-Facility Specialists, and Statewide Transportation Services.Albuquerque Ambulance Service (AAS) offers continuing and community education courses that are open to the public including CPR / BLS, ACLS, PALS, TFR and more!/GEMS Statement Request (PCS) for Txp/PCS For Ambulance 1-800-658-6009 Transport fax 888-586-9105. Complete ALL sections of this form. To meet this requirement, the patient must be either “bed confined” or suffer from a condition such that transport by means other than an ambulance is contraindicated by the patient’s condition. The completed form should be faxed to PINELLAS COUNTY EMS D/B/A SUNSTAR at: (727) 582-2540 SUNSTAR AMBULANCE DISPATCH PHONE: (727) 587-2111 Ver. Chicago 773-429-8880.☐Gurney/litter/stretcher van ☐ BLS ambulance ☐ ambulance Critical care transport ☐ transportation Wheelchair van These services require physician justification and . Medical Record and Billing Release Policy. Registered Nurse.If this box is checked, I also certify that the patient is physically or mentally incapable of signing the ambulance service’s claim form and that the institution with which I am . FACILITY REPRESENTATIVE - COMPLETE .37, the specific reason(s) that the patient is physically or . Maryland MOLST Form.If patient is a repetitive patient, complete the repetitive patient PCS form.AAS welcomes the opportunity to provide general health education and injury prevention programs for our community and charitable organizations.☐Gurney/litter/stretcher van ☐ BLS ambulance ☐ ambulance Critical care transport ☐ transportation Wheelchair van These services require physician justification and signature below. Ambulance providers are required by federal regulations (Code of Federal Regulations, §410. The Check boxes are provided to assist the physician or authorizing party in describing the medical situation requiring the use of an ambulance.
Albuquerque Ambulance Services

Forms & Documents–Patients & Family Members Medicare - Elite Ambulance.
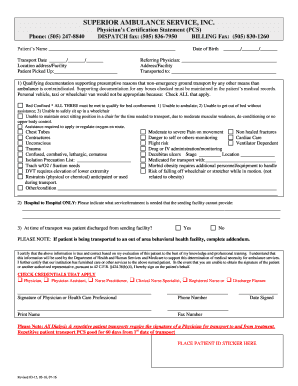
PHYSICIANS CERTIFICATION STATEMENT
NOTICE: It is federal mandate that ALL non-emergency . Call us today at (847) 816-4600. NW Indiana 219-322-6061.40 (D) (2) and (D) (3). Home ; About Us; Services. Which assists in the . supervised protective restraint. Medicare memo PM AB-99-53 states that a physician’s certification statement can be signed PA, CNS, NP, RN, or Discharge Planner if the physician is unable to sign. Skokie, IL 60076 . Beneficiary Signature Form. Email: info@lifelineamb. Main Office 3737 Chase Ave. Box 98000 LAFAYETTE, LOUISIANA 70509 -8000 1 -800 -259 -2222 I. Is this patient “bed confined” as defined below? reason(s) that the patient is physically or mentally incapable of signing the claim form is as follows. Patient’s Name: Date of Birth: ___________ Medicare #: Transport Date*: .Quick forms that you can fill out, download, & print for Patriot Ambulance.
Physician Certification Statement Form
Suburbs 708-478-8880.Taille du fichier : 284KB
Ambulance physician certification statement
Physician certification statements (PCS) are required for patients who are under the direct care of a physician and are required for: Scheduled non-emergency . 40 (d) a Physician Certification Statement (PCS) from the patient’s attending physician for nonemergency ambulance transportation.
ALBUQUERQUE AMBULANCE SERVICE
Physician’s Certification Statement for Ambulance Transportation (PCS) The completed form should be faxed to MedStar Mobile Healthcare at: (817) 632-0537 Communications . Physician’s Medical Necessity Certification for Non-Emergency Ambulance Transports. To schedule NMT, AA NEMT, or authorized NEMT, please call L. Non-Emergency Ambulance Transportation.
Microsoft Word
AMR Personnel may not complete this section.
Physician’s Certification Statement (PCS)
AMBULAN CE TRANSPORTATION IS MEDICALLY NECESSARY . Fax: 434-634-1155 Physician Certification Statement for Non-Emergency Ambulance Services – v112016 . Emergency; Non-Emergency; Healthcare Systems; Special Events; Careers; Forms; Contact Us; Forms. Transportation Request – Hospital.